
Footprints that leave no footprints. Credit: Adam Scott CC
The reorganisation of health services in England by teams of planners in 44 “footprints” could hardly be more important, yet the process has no legal basis. This means a corresponding lack of public accountability, increasing the risk of serious mistakes, conflicts of interest and misuse of public funds.
Evidence of how serious this is comes from two attempts to ascertain some of the costs of the planning process, using Freedom of Information (FoI) requests addressed to each of the 44 STP teams. One was by the GPs’ journal Pulse. Pulse asked what was the cost of external consultants. Although public bodies are required to respond to FoI requests within 20 working days, Pulse reported receiving only 19 responses (43%). The CHPI also asked for the costs of employing external consultants, and after an arduous process of enquiry eventually received 36 responses (82%). Eight STP teams which responded to both Pulse and the CHPI sent different data to each. Sometimes the data differed by as little as five per cent but some differed by as much as 300%. In other words the responses, besides being incomplete, do not give a reliable overall picture of how much STP teams are spending on external consultants.((Pulse extrapolated the average (mean) spend on external consultants for the 19 STPs which responded to their request to arrive at a total spend of £21m for all 44 footprints. This is not very different from an equivalent extrapolation from the 36 responses of £24m, but the responses seem too unreliable to support the claim that this is what has actually been spent on management consultants.))
The data do nonetheless show that some STP teams have spent large sums on external consultants, from the £678,000 spent by Staffordshire and Stoke to the £3.2 million spent by Kent and Medway. It will be interesting to see how far this results in superior planning and an improvement in services to patients, as promised in the Five Year Forward View. Analysis of the emerging plans by the CHPI and others has so far not been encouraging in this regard.
The CHPI also asked for the spending on NHS staff involved in the planning process. Six STPs reported that no NHS staff time had been used, and twelve could not supply a figure or a numerical estimate, or said they did not hold specific data. The remaining eighteen reported spending an average of £523k (with a median of £260k) on NHS staff working on STP planning from January 2016 to March 2017. Some reported as little as £66k while two reported spending over £1m, and one (South East London) reported spending £2,147,000. It should be noted, however that these larger figures probably reflect more diligent accounting of NHS staff time by these STPs than excessive spending. The wide discrepancies probably also stem from a variety of other causes, including the likelihood that some respondents regarded the work done by Commissioning Support Units as NHS staff time, while others did not. In general, the variation in the reported data for time spent by NHS staff on planning implies that there is no shared understanding of the costs of planning on the part of many if not most STP teams.
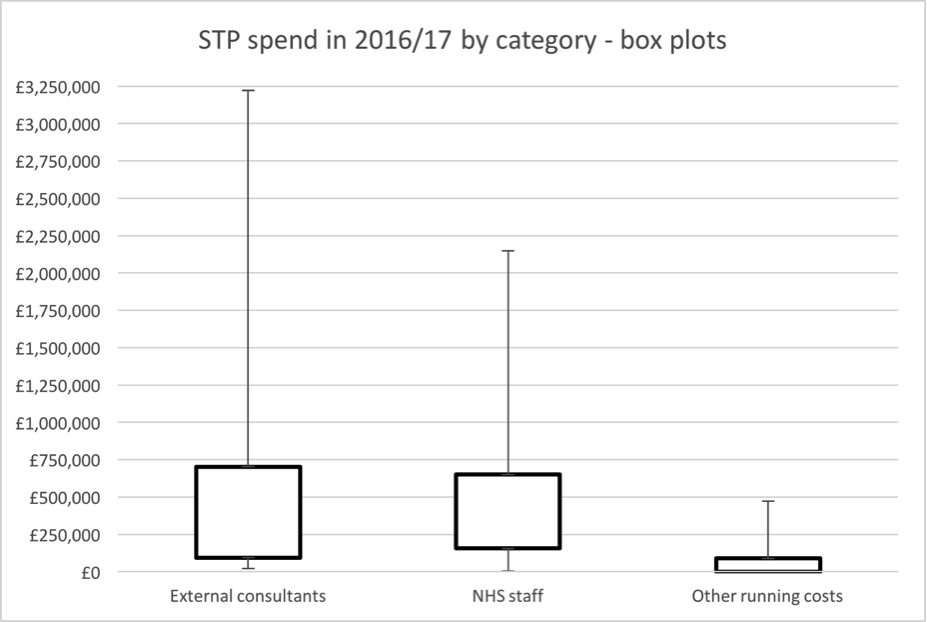
As the box plots (Chart 1, below) show there are large variations in the reported amounts spent on external consultants, NHS staff, and other running costs (the boxes represent the spend by the middle 50% of STPs). For example, for external consultants the gap between the 75th and 25th percentiles is £609,000. When the full range of responses are included the gap between the highest and lowest spending STPs widens to just under £3.2m.
Chart 1. STP spend in 2016/17 by category
A more realistic picture of the overall costs of producing STPs might be gained from looking at the estimates of the combined cost of external consultants, NHS staff, and other non-staff spending for the next year of planning, 2017-18. The CHPI requested this information in late March 2017. Twenty-four STPs reported that they did not yet have, or could not supply, a budget for 2017/18. The twelve which did report budgets expected to spend an average of £1.0m on external consultants, NHS staff and non-staff items combined, with a median of £695k – almost the same as the previous year’s median combined total of £687k for the 36 STPs which responded to our requests.
Table 1. 2017/18 STP budgets (reported)
| Name of Footprint | STP 2017/18 budget (consultants, staff time, other running costs) |
| South East London | £3,359,000 |
| Staffordshire and Stoke on Trent | £2,460,815 |
| Cornwall and the Isles of Scilly | £2,000,000 |
| Norfolk and Waveney | £1,010,000 |
| West Yorkshire and Harrogate | £886,000 |
| Somerset | £860,170 |
| Bath and North East Somerset, Swindon and Wiltshire | £530,500 |
| Humber, Coast and Vale | £400,000 |
| West, North and East Cumbria | £400,000 |
| Hampshire and the Isle of Wight | £287,013 |
| Suffolk and North East Essex | £200,000 |
| Lincolnshire | £173,000 |
Extrapolating the average budget of these twelve STPs to all 44 footprints would imply a total cost of planning in 2017-18 of £46m. However, the amounts of budgeted expenditure by these twelve STPs ranged from as little as £173k to as much as £3.4m. Since the planning challenge facing all STP teams is more or less the same, these widely varying data also seem unlikely to be a good indication of what will actually be spent in all of these footprints.
The difficulties in obtaining complete and reliable data from STP teams and the significant variations in their responses reflect the inherently unaccountable nature of the STP planning process. Under the Health and Social Care Act 2012 Parliament has no oversight of the management of the NHS, and local oversight by local authority Scrutiny Committees has been made ineffective by the transfer of decision- making from CCGs to STP partnerships. Unless these partnerships are given a legal basis with clear rules on transparency it will not possible for the public to find out exactly what is being done to the NHS or to hold the planners to account for it.
Support Our Work
CHPI is the only truly independent health think-tank dedicated to the founding principles of the NHS. To continue our work keeping the public interest at the centre of health and social care policy, we need your help.
Please support CHPI so we can continue to impact the health policy debate.